Welcome to the Long-Term Consequences of British Colonization on the Public Health of India research guide! This project was created as part of the Richter Library's Research Scholar's Program. My name is Josh Patel, and I will be graduating Spring 2025 with a BS in Neuroscience. My interest in medicine influenced my idea for this project to highlight the otherwise overshadowed genetic health disparities in my own community that arise from decades of subjugation from British colonialism. My primary goal for this project was to bring awareness to how colonialism and policy can affect health issues such as diabetes and cardiovascular disease.
Thank you,
Josh Patel
Read my Bibliography!
You can read my bibliography at scholarship@miami for more information!
How British Colonialism Increased Diabetes in South Asians
This video reveals how South Asian communities have elevated the rates of diabetes compared to almost every other population. Prior to recent research, the blame was put on South Asian diets not being nutritionally filling, leading to the development of diabetes in young adults. During the period of the British Raj, there were 25 major famines that directly killed 60 million people in a span of 60 years. However, in the two thousand years prior to British arrival, there were only 17 recorded famines. During the war effort, Winston Churchill’s exploitative policies stripped Indians of food and water, directly causing the Bengal famine, and killling over 3 million. Even though these famines were decades ago, epigenetics continues to play a huge role in how South Asian bodies store fat to make these populations famine resistant, which in turn makes the subsequent generation twice as likely to develop diabetes, high blood glucose, and countless other chronic conditions. Due to the considerable number of famines that the population had lived through in recent modern history, some of which are listed below, the rates of diabetes and cardiovascular disease in particular has skyrocketed.
British India - 1947
August 14, 1947 - Uttar Pradesh, India
Indian Poverty and Malnutrition
Prior to English colonization, India was ruled by the Mughal Empire and suffered wages below sustenance - defined as the income sufficient to support a family of four at 2,000 calories per person per day - once during the Deccan famine between 1630-1632 (Winter et al., 2017). However, once India was under full British control and forced into its capitalist world-system, famines and foreign policy combined led to almost a full century of wages below sustenance (Sullivan & Hickel, 2023). This lack of sustenance did not change until India received independence (Sullivan & Hickel, 2023). Robert C. Allen, a reviewer in the annual review of economics from 2020, revealed that poverty increased under British rule, claiming “imperialism and globalization must have played leading roles” in the unemployment and poverty in India today.
Furthermore, data from the bodies found at the Ancient Harrappan burial site (an indigenous community that thrived between 3300 - 1300 BCE) shows their average height to be around 169 cm or 5’6”. Meanwhile, countries under British control were on average a minimum of 2-3 inches shorter until around 1870. Around 1870, however, a series of British policies led to widespread famine that reverted the progression until the mid to late 20th century, after India received its independence. Height is often used as an indicator of societal public health during excavations of ancient burial grounds, as it is often times the only biological data that can be calculated quickly without long-term genetic analysis (Clark 2007).
Healthcare Inequities in India
Healthcare availability and quality in India today has been shaped for decades by British occupation (1757-1947). The occupation brought with it a shift in medicine from Eastern traditional practices, focused on maintaining health and preventing disease, (ex. Aryuvedic practices), to Western innovations, such as surgical intervention. During colonial rule, healthcare availability was incredibly poor, with superior healthcare services reserved solely for European occupants, meanwhile native Indians received poor quality healthcare treatments. After achieving independence in 1947, India rapidly developed its urban healthcare in favor of the remaining elites, whereas rural and underprivileged populations continued to suffer from higher mortality rates and poor access to healthcare. Furthermore, healthcare privatization in the early-mid 1980’s only exacerbated the issue, leaving almost 800 million individuals with low quality services and long waiting times (Mustaq, 2009). Modern programs such as National Health Missions and government-subsidized insurance has emerged to address the issues, but challenges remain, particularly the concern that healthcare costs in India will soon rise to match that of the United States.
Early British Colonialism
Painting of India under Colonial Rule - 1752
The Bengal Famine
Ration lines during the 1943 Bengal Famine.
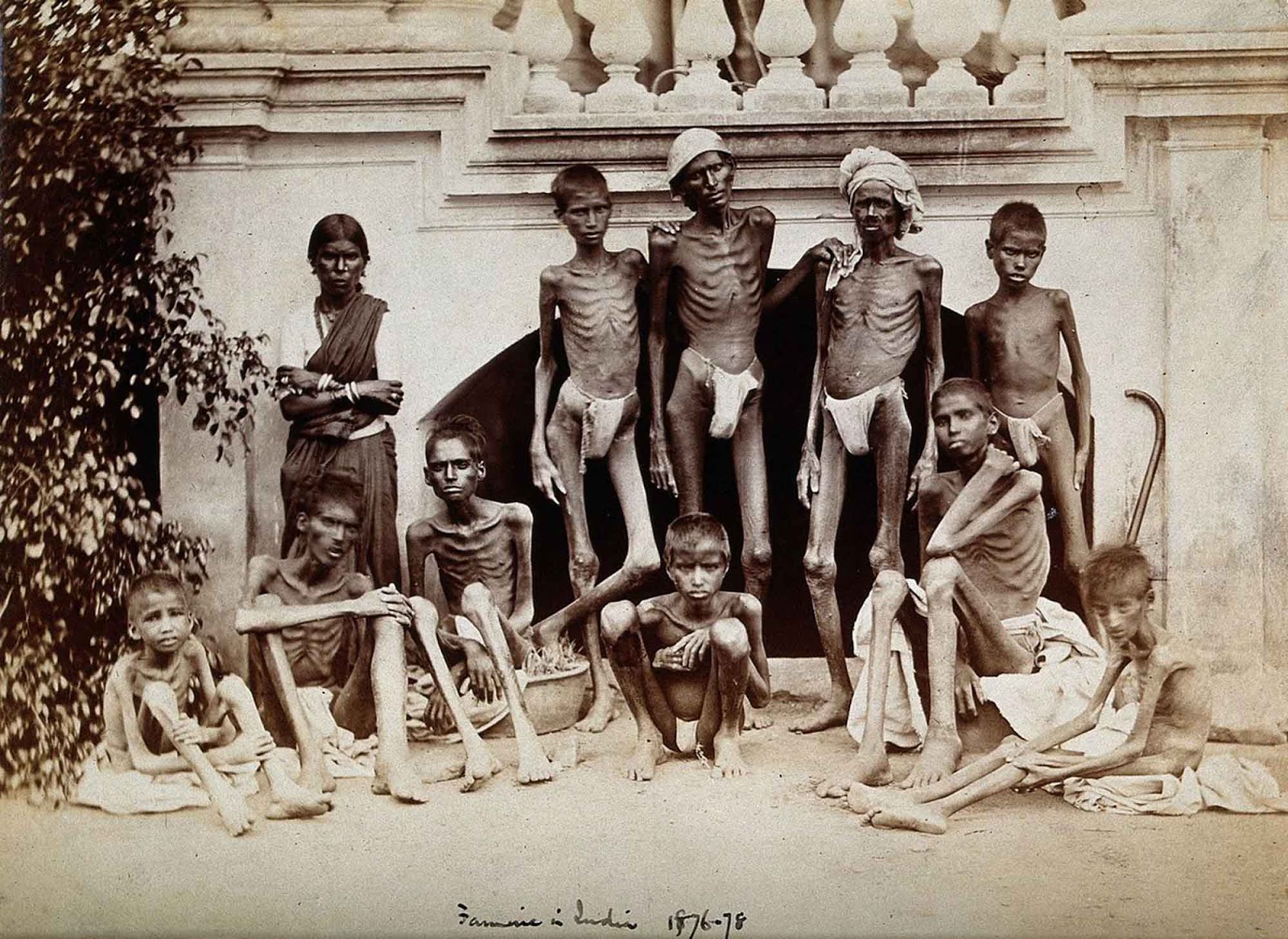
The Madras Famine
A family during the Madras Famine - 1876
A Few of the Major Famines Suffered in India
1. Great Bengal Famine (1770)
Death toll: Estimated 10 million (about one-third of Bengal's population).
Regions Affected: Bay of Bengal
Cause: A mix of crop failure and brutal tax policies under the East India Company (heavily backed by the British government). Despite the famine, taxes were still collected, and grain was exported.
2. Madras (South India) Famine (1876–1878)
Death toll: 5.5 to 10 million.
Regions affected: Madras - Southern India
Cause: Drought, combined with rigid colonial economic policies. Despite food scarcity, grain continued to be exported to Britain. Relief efforts were minimal and delayed.
3. Great Famine of 1896–1897
Death toll: About 5 million.
Regions affected: Central and Northern India.
Cause: Monsoon failure, crop failure, and inadequate relief efforts. British policies prioritized market prices over emergency aid.
4. Indian Famine of 1899–1900
Death toll: 1 to 4.5 million.
Regions Affected: Western and Southern
Cause: Drought and locust infestations. Relief was often conditional, and famine camps had harsh requirements for aid.
5. Bengal Famine (1943)
Death toll: 2 to 3 million.
Regions Affected: Bay of Bengal - East India
Cause: Disruptions caused by World War II such as hoarding, rice exports, and British wartime policies under Churchill’s government. Grain was stockpiled for the war effort while locals starved.
"The Last Effort and Fall of Tippoo Sultaun" - Henry Singleton, c. 1800
Diabetes and British Colonialism
British colonial policies in India significantly altered the nation's agricultural practices, dietary habits, and urbanization patterns, laying the groundwork for the current diabetes epidemic. The colonial emphasis on cash crop cultivation for export, such as indigo and cotton, reduced the land's availability for staple food production, leading to food insecurity and malnutrition among the local population whenever droughts arose, and therefore leading to wide-scale famine. Colonial policies led to the erosion of traditional diets and lifestyles, replacing them with sedentary labor systems and diets aligned with industrial and urban economies. These shifts disproportionately affected lower-income populations, who inherited both poor living conditions and limited access to quality healthcare. Moreover, British infrastructural development was highly unequal—prioritizing trade and resource extraction over local public well-being. This contributed to persistent health inequities that left millions vulnerable to lifestyle and stress-related diseases. The failure to establish a robust public health system under colonial rule has had lasting consequences on India’s ability to respond to its current cardiovascular health crisis. These factors collectively disrupted traditional diets and increased the risk of metabolic disorders among south-east Asian populations.
The legacy of these colonial policies is evident in the current prevalence of diabetes in India. For instance, urban areas in India exhibit higher rates compared to rural regions, reflecting lifestyle changes associated with urbanization. Furthermore, due to the lack of healthcare access across the nation, a significant portion of individuals remain undiagnosed. For example, in Delhi, India, 17.5% of cases were undiagnosed as of 2011 (Pradeepa 2021).
The increased susceptibility of South Asians to type 2 diabetes, even those within a normal range of body mass index (BMI), can be partly attributed to genetic factors. Research indicates that South Asians, particularly Asian Indians, have a greater genetic predisposition to impaired insulin secretion, making them more prone to developing diabetes at a younger age . This genetic vulnerability, combined with the environmental and lifestyle changes initiated during the colonial era, has contributed to the high rates of diabetes burdening India today.
Diabetes Infographic
The Burden of Diabetes in India - Research Gate, IDF Diabetes Atlas 2019
The Kohinoor Diamond
The Kohinoor Diamond, one of the most famous examples of artifacts being stolen by the British Empire. It was taken following the conquest of Punjab (Northern India) in 1849, and is valued from anywhere between $140 to $400 million according to Kate Ng of the Independent.
Economic Exploitation Under British Colonialism
British colonialism had a profound impact on India's economic landscape, that lead to the country's widespread poverty that persists to this day. Between 1765 and 1900, Britain is estimated to have drained approximately an astronomical $45 trillion from India (Chakrabarti & Patnaik, 2019) This finanical extraction was facilitated through policies that prioritized British interests, such as the deindustrialization of India's textile industry and the imposition of high taxes on Indian peasants. The British also implemented systems like the salt tax, which inflated teh cost of essential goods and contributed to widespread deprivation, best exemplified by the Great Hedge of India. The cumulative effect of these policies was a significant decline in India's share of global industrial output, from 25% in 1750 to just 2% by 1900 (Clingingsmith & Williamson, 2004). Moreover, the export of raw materials from India, including the Kohinoor Diamond (picture on the left), deprived the country of it's own resources that could have been better used to develop its own industries and public health infrastructure.
The economic policies implemented during British colonial rule had a detrimental effect on India's health system. For instance, the British allocated a significant portion of India's revenue to fund military expenditures, both within India and abroad, rather than investing in healthcare or education. In 1943, the Health Survey and Development Committee, led by Sir Joseph Bhore, reported that India had approximately 7,400 hospitals and dispensaries, with a bed population ratio of 0.24 per 1,000 people. This was substantially lower than the global average at the time, indicating a significant gap in healthcare provision. Additionally, the number of qualified medical professionals was limited; there were only about 47,000 doctors and 7,000 nurses across the country. The British administration's policies prioritized the health of European settlers and military personnel over that of the indigenous population, leading to disparities in healthcare access and quality. Furthermore, traditional Indian medical systems like Ayurveda and Unani were marginalized, while Western medicine was promoted, often without integrating beneficial aspects of indigenous practices. The long-term impact of these colonial policies is evident in the ongoing challenges faced by India's health system, including disparities in healthcare access and outcomes.
2. Wells, J. C. K., Pomeroy, E., Walimbe, S. R., Popkin, B. M., & Yajnik, C. S. (2016). The Elevated Susceptibility to Diabetes in India: An Evolutionary Perspective. Frontiers in Public Health, 4, 145. https://doi.org/10.3389/fpubh.2016.00145
5. Panda, K. (2023, May 18). The Effects of Direct and Indirect Colonial Rule on Health Outcomes in India. https://www.sciencespo.fr/ecole-recherche/sites/sciencespo.fr.ecole-recherche/files/Master-Thesis_Kunal-Panda.pdf
7. Mushtaq, M. U. (2009). Public Health in British India: A Brief Account of the History of Medical Services and Disease Prevention in Colonial India. Indian Journal of Community Medicine : Official Publication of Indian Association of Preventive & Social Medicine, 34(1), 6. https://doi.org/10.4103/0970-0218.45369
8. Sullivan, D., & Hickel, J. (2022, December 2). How British colonialism killed 100 million Indians in 40 Years. Al Jazeera. https://www.aljazeera.com/opinions/2022/12/2/how-british-colonial-policy-killed-100-million-indians
10. Pradeepa R, Mohan V. Epidemiology of type 2 diabetes in India. Indian J Ophthalmol. 2021 Nov;69(11):2932-2938. doi: 10.4103/ijo.IJO_1627_21. PMID: 34708726; PMCID: PMC8725109.
12. Clark, Gregory. A Farewell to Alms: A Brief Economic History of the World, Princeton: Princeton University Press, 2008. https://doi.org/10.1515/9781400827817
13. Chakrabarti, S., & Patnaik, U. (2019). Agrarian and other histories: Essays for Binay Bhushan Chaudhuri.
14. Clingingsmith, D., & Williamson, J. (2004). India’s De-Industrialization Under British Rule: New ideas, new evidence. https://doi.org/10.3386/w10586

:quality(75)/https%3A%2F%2Fassets.lareviewofbooks.org%2Fuploads%2F201809BritishRaj.png)